Insights & Perspectives
Clinical Utility Is the Bridge Between Science and Adoption
Scientific validation and clinical validation create credibility. Clinical utility is what connects a diagnostic test to real-world decision-making, reimbursement, adoption, and commercial value.
Scientific validation and clinical validation create credibility. Clinical utility is what connects a diagnostic test to real-world decision-making, reimbursement, adoption, and commercial value.
Scientific validation and clinical validation are essential in diagnostics.
They establish whether the biology works, whether the assay performs, and whether the test is meaningful in the intended clinical population. Without that foundation, a diagnostic test has no credible path to adoption.
But scientific and clinical validation are not the same as clinical utility.
Clinical utility asks a more practical question:
Does using this test change what happens next?
That question is central to diagnostics commercialization.
A diagnostic test may be analytically sound, scientifically interesting, and clinically validated, yet still struggle to gain market adoption if it does not clearly influence patient management, treatment selection, risk stratification, workflow, cost, or clinical decision-making.
In diagnostics, evidence has to do more than prove that a test performs. It has to support why the test should be used.
The Clinical Utility Bridge
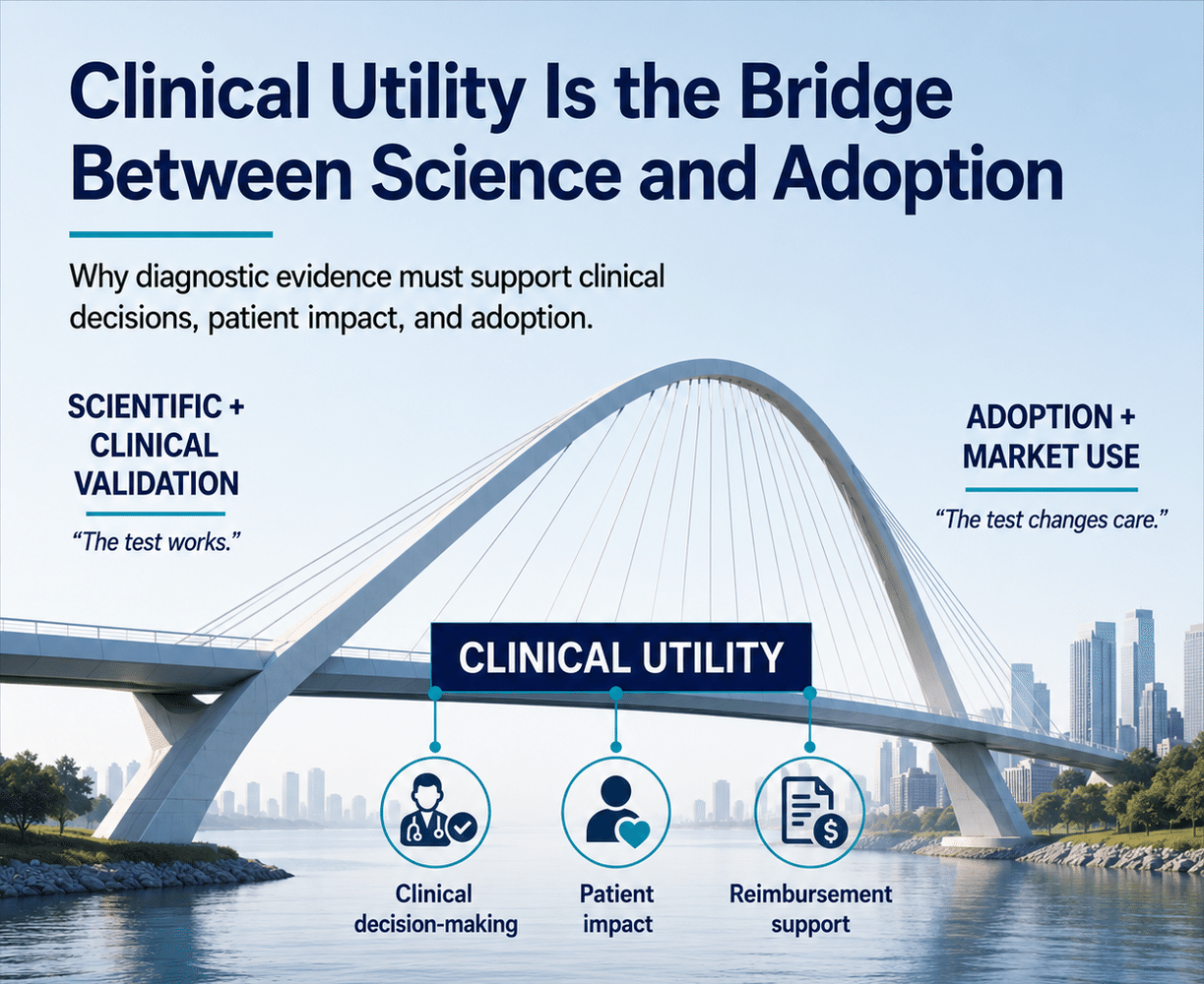
Clinical decision-making
Does using the test change what the clinician does next?
Patient impact
Does the test improve patient management, outcomes, or care?
Reimbursement support
Does the evidence justify coverage and payment?
Three Different Evidence Questions
Diagnostics companies often describe evidence broadly, but the evidence questions are distinct.
Scientific validation asks:
Does the biology work?
Clinical validation asks:
Does the test perform in the intended clinical population?
Clinical utility asks:
Does using the test improve clinical decision-making, patient management, workflow, outcomes, or healthcare economics?
These layers are related, but they should not be blurred together.
Scientific validation creates credibility. Clinical validation creates confidence. Clinical utility creates relevance.
That relevance is what connects the test to the healthcare system.
Why Clinical Utility Matters Commercially
Clinical utility matters because diagnostics are rarely adopted simply because they produce interesting information.
Physicians, laboratories, payers, health systems, and patients each need to understand what the test changes.
- Does it help select therapy?
- Does it reduce unnecessary procedures?
- Does it identify the right patient earlier?
- Does it avoid ineffective treatment?
- Does it improve monitoring?
- Does it support a more appropriate referral?
- Does it reduce downstream cost?
- Does it make care more precise, practical, or measurable?
Those questions are not only scientific. They are commercial.
They shape reimbursement strategy, physician adoption, payer confidence, health-system acceptance, and investor confidence.
A test that performs well but does not change care may be clinically interesting. A test that changes care has a stronger path to adoption.
"Clinical utility is where diagnostic science becomes commercially relevant."
Clinical Utility Should Shape Development Early
Clinical utility should not be treated as a late-stage claim added after validation.
It should inform development from the beginning.
If the intended use case is unclear, evidence generation may drift toward data that is scientifically credible but commercially incomplete. A company may produce strong analytical performance, generate peer-reviewed publications, and still fail to answer the questions that determine whether the test will be ordered, reimbursed, and adopted.
The right questions need to be asked early:
- What clinical decision is the test intended to influence?
- Which patient population matters most?
- What comparator is relevant?
- What outcome or management change should be measured?
- What evidence would create physician confidence?
- What evidence would support payer coverage?
- What economic value could justify reimbursement?
- What workflow must the test fit into?
- What would cause the program to advance, change, partner, pause, or stop?
These questions help determine whether the company is building evidence for adoption, not only evidence for scientific credibility.
Clinical Utility and Reimbursement Are Connected
Payers are not simply asking whether a diagnostic test is novel or technically valid.
They are asking whether the test changes clinical management in a way that justifies payment.
That does not mean every diagnostic must prove a direct outcome benefit in the same way a therapeutic might. But it does mean the company needs a credible argument that connects the test result to a meaningful clinical action, patient management decision, or healthcare value.
A reimbursement strategy built only on analytical performance is usually incomplete.
Coverage often depends on whether the test helps answer a meaningful clinical question, whether the result changes what happens next, and whether that change supports a reasonable payment model.
Clinical utility is the evidence bridge between test performance and payer value.
Clinical Utility and Physician Adoption Are Connected
Physicians may understand the science and still hesitate to order a test if the result does not clearly support a decision.
The test has to answer a question that matters in practice.
If the result does not change therapy, monitoring, referral, follow-up, risk assessment, or patient management, adoption may remain limited. Physicians already operate within time constraints, ordering systems, payer requirements, patient cost concerns, and established care pathways.
A diagnostic test has to earn its place in that environment.
Clinical utility helps make the test practical. It gives the physician a reason to order it, interpret it, explain it, and act on it.
Clinical Utility and Commercial Execution Are Connected
Even strong clinical utility does not implement itself.
A company still needs a commercial model that explains the value clearly, supports physician education, addresses payer requirements, enables ordering, supports reporting and interpretation, and measures adoption.
Clinical utility creates the basis for adoption. Commercial execution turns that basis into a repeatable business process.
That distinction matters.
A diagnostics company may have a compelling clinical utility story but still underperform commercially if the field team cannot communicate it, if the ordering process is burdensome, if reimbursement is uncertain, or if the company lacks a disciplined adoption model.
The strongest companies connect clinical utility to every part of the commercialization plan: evidence generation, reimbursement strategy, customer segmentation, messaging, sales process, workflow support, and performance metrics.
The Bridge Between Science and Adoption
Clinical utility is where diagnostic science becomes commercially relevant.
- It connects technical performance to clinical action.
- It connects clinical action to payer value.
- It connects payer value to market access.
- It connects market access to adoption.
- It connects adoption to commercial scale.
That is why clinical utility should not be treated as a supporting detail. It is one of the central design questions in diagnostics commercialization.
For diagnostics companies, the essential question is not only whether the test works.
The stronger question is: If the test works, what will it change?
That is the bridge between science and adoption.
Life Science Dx Consulting helps diagnostics companies translate clinical utility into reimbursement strategy, physician adoption, workflow fit, and scalable commercial execution.
Let's Talk
Continue the Discussion
Life Science Dx works with diagnostics and life science companies to build the clinical utility evidence, reimbursement strategy, and commercial execution model needed to move from science to adoption.